Team:KCL UK/Description
Project Description:
Project Inspiration:
The inspiration for our project, Renervate, can be traced back to iGEM 2019. During their time at the Giant Jamboree, our Team Leaders attended two pivotal presentations that would shape King’s College London’s 2020 project. Firstly, they attended Leiden’s presentation which revealed to them the potential of using protein-based hydrogels to treat burn wounds. Their project employed suckerin, a protein derived from the Humboldt squid, Dosidicus gigas. Not only were they incredibly impressed by their amazing presentation, but by how their team looked to unsuspecting sources to develop a novel biomaterial approach to a seriously debilitating condition. Secondly, they attended the presentation by SCIE Great Bay whose project focused on categorising numerous mussel foot proteins (MFPs) with the intent of their use as bioadhesives. Particularly, they were fascinated by the potential applications of using MFPs in therapeutics, which their team touched upon. While watching these two presentations, our Team Leaders were able to draw connections between them and thus begin to shape our project. From here, our newly formed team decided to research MFP-based biomaterials and their applications.
Defining the Problem:
To begin, we needed to determine how a potential product could be applied to a particular problem. As our team has a very strong biomedical background, we decided to look into the therapeutic uses of MFPs and biomaterials in general. Based on this general research, it became clear to us spinal cord injury (SCI) is a serious condition that could potentially be solved using a biomaterial and Synthetic Biology based approach (Straley et al., 2010). SCI is caused by trauma to the spinal cord such as compressions, lacerations, and contusions (Katoh et al., 2019) that damages both neural and vascular systems. The initial mechanical injury causes on onset of the acute phase of the SCI, later progressing to the sub-acute and chronic stages (Silva et al., 2013). The sub-acute phase is characterised by numerous biological events that include but are not limited to vascular changes, free radical formation and lipid peroxidation, apoptosis, glutamate excitotoxicity, disruption of ionic balance, and a profound immune response (Silva et al., 2013). The shift into the chronic phase is distinguished by the formation of a glial scar, which acts as a physical barrier to axonal regrowth. The severing of the axons and the formation of the glial scar disrupts the flow of information to and from the brain and the body leading to either partial or complete loss of sensation below the level of injury. Paraplegia, quadriplegia, and tetraplegia are all possible clinical outcomes of SCI and have severe economic, physical, and mental effects on the individual.

Despite the severity of the clinical demonstrations of this condition, there is no cure for spinal cord injury. Although numerous treatments exist, they primarily focused on management and rehabilitation, not curation. In the United Kingdom, there are over 50,000 people currently living with SCI (Patek and Stewart 2020), and in the United States that number is nearly four times as high with a staggering 288,000 persons living with the condition [as of 2018]. What’s more, these numbers are predicted to grow. In the United States alone, there are approximately 17,700 new SCI cases each year. The global incidence of SCI has seen a rise the last few decades due to an increase in the ageing population and increase in falls and traffic accidents (Badhiwala et al., 2018). Beyond the physical effects, SCI places a formidable burden on the economic and mental well-being of the individual. Nearly 48.5% of patients diagnosed with spinal cord injuries suffer from mental health problems; including depression, anxiety and PTSD (Migliorini et al., 2008). Additionally, the average lifetime cost of health and social care for a person with a spinal cord injury in the UK is £1.12 million (McDaid et al., 2019). The economic, physical and mental devastation caused by SCI cannot be understated. Despite the increase in success and access to care worldwide, the repercussions of SCI continue to pose a serious global challenge. Based on our research, we identified a clear problem and were inspired to look for solutions.

Developing our Ideas:
In doing so, we found that we were able to incorporate our original ideas inspired by Leiden and Great Bay SCIE. Our preliminary research demonstrated to us that the main way in which biomaterials have been proposed as a treatment for SCI is as a bridging construct that facilitates axonal regrowth (Shrestha et al., 2014). The biomaterial “bridge” is referred to as a scaffolding and is used to restore tissue continuity in the injured area. Scaffolds intended to be used in SCI treatment can be split into two categories: hydrogels and nerve guidance channels. The former are “hydrophilic, three-dimensional networks that are able to absorb large quantities of water or biological fluids” (quote from Chai et al., 2017). Hydrogels show great promise as they are injectable, flexible, and can be easily modified to contain elements that encourage nerve regrowth, such as biomolecule delivery and cell encapsulation (Straley et al., 2010). On the other hand, nerve guidance channels are channels that direct nerve growth from the proximal to distal nerve stumps and prevent regrowth into the scar. Similarly, nerve guidance channels can be designed to optimise regeneration by careful selection of macroarchitecture and microarchitecture features. With regards to SCI, hydrogels have been shown to be very promising as a consequence of their injectability, facilitating a much simpler implantation process in light of the complex geometries of the wound site. However, hydrogel technology still has far to come with regards to mechanical strength, degradation, cell-adhesivity, and topography. Therefore, our team decided to look into nerve guidance channel-based scaffolds, which have been shown to have the mechanical and physical properties required for implantation in the spinal cord. As a consequence, our team decided to research further into the design and modelling of a 3D bioprintable scaffold for the treatment of SCI.
Project Overview:
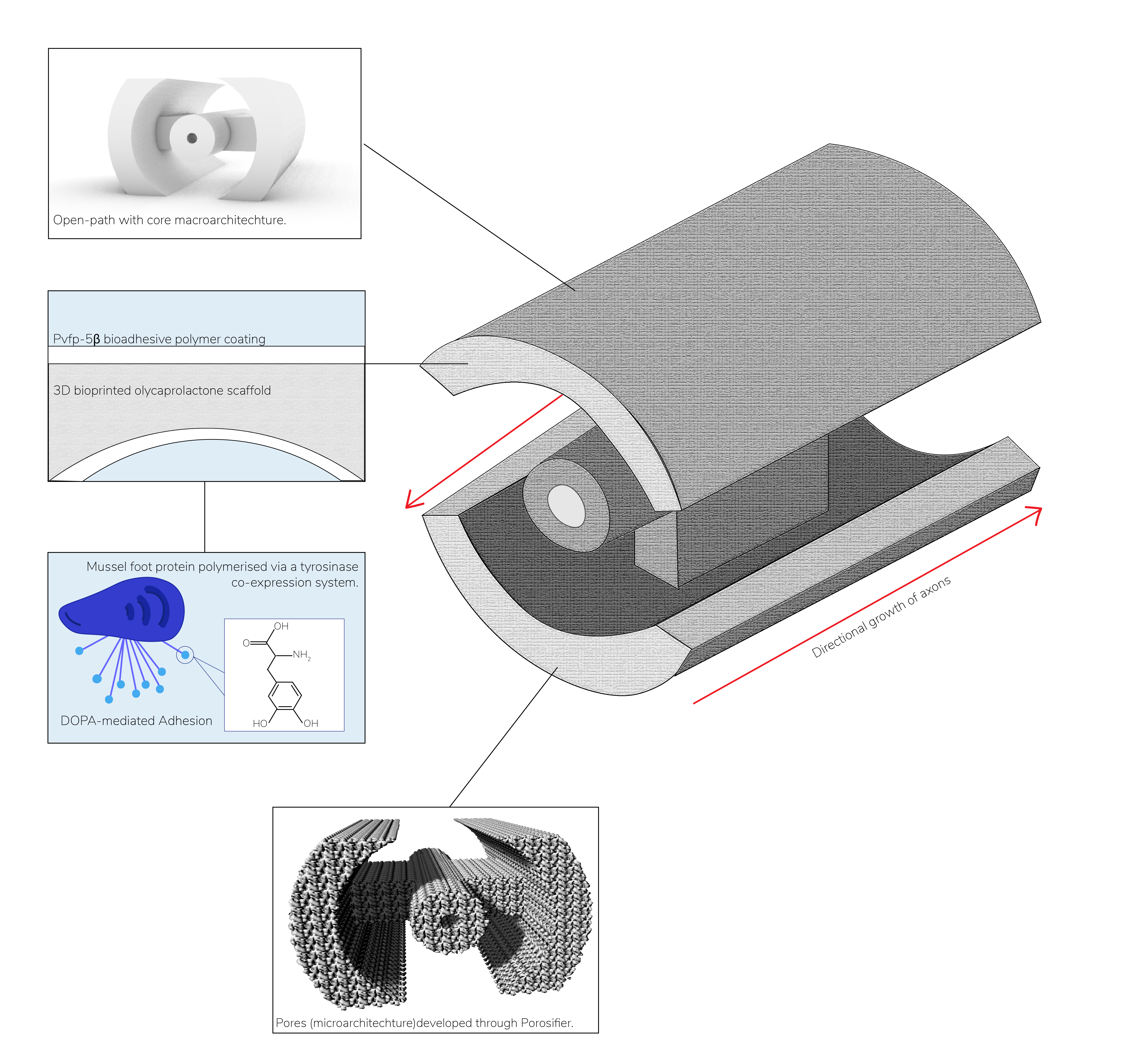
The Phase I project of Reneverate is focused on the design and modelling of a 3D-bioprinted polycaprolactone (PCL) based scaffolding that contains a novel mussel-foot protein based bioadhesive coating formed by Pvfp-5β. The second phase of our project will consist of the wet lab validation and formation of the scaffolding and the protein polymer. Our MFP coated scaffolding design has numerous potential applications in tissue engineering, yet we have designed it for use in treatment of SCI. The aim of our project is to outline a holistic, less invasive treatment that reduces the need for surgical intervention and focuses on functional restoration rather than management. To do so, we have designed an alternative method of glial scar removal prior to scaffold implementation and have carried out rational protein design to develop a novel, synthetic fusion protein that aims to encourage axonal regeneration in the spine. Furthermore, we have designed a biodegradable and biocompatible scaffolding that has been shown to withstand the mechanical forces of the spine and have modelled its degradation rate to ensure that it will remain in the spine for long enough to ensure healing without. Beyond the scientific aspects of our project, we have examined the societal role in SCI treatment. Consequently, Renervate has developed a Human Practices and Science Communication plan that ensures that we are able to tackle the social side of the problem.
Project Goals:
- Research into SCI pathophysiology and axonal regeneration to understand how to best design a scaffold that encourages regrowth via topography.
- Carry out a literature search into pre-existing macroarchitechture designs. Generate computer-aided design (CAD) models of five macroarchitectures using the Autodesk Inventor Software. CAD models will be specific to a patient and will be developed based on the obtained MRI scans.
- Determine which macroarchitechture is most suitable for our purposes using Finite Element Analysis (FEA) with the Autodesk Inventor NASTRAN software.
- Demonstrate the applicability of the chosen macroarchitechture by simulating the design under a real-life condition.
- Carry out a literature review into potential scaffold micro architectures and their respective abilities to topographically stimulate nerve regeneration.
- Provide a model that predicts the degradation rate of the PCL-based scaffold, therefore determining the molecular weight needed to ensure the scaffold remains in the body for the duration of healing.
- Using Molecular Dynamics (MD) simulations and GROMACS, provide a structural model for our chosen MFP, Pvfp-5β. In doing so, we can understand our protein further.
- Once the structural model is complete, using YASARA software to examine the structural and physicochemical properties of Pvfp-5β.
- Build upon the
- Carry out literature search into the process by which we can develop a genetic system to polymerise our protein in vitro.
- Write up protocols for the following experimental work that will take place next year: polymerisation and purification of Pvfp-5β, testing immunogenicity and cytotoxicity of the Pvfp-5β polymer, coating the 3D bioprinted PCL scaffold with the Pvfp-5β polymer, examining the absorption of the protein polymer into the surface of the PCL scaffold, determine the adhesive performance of the encoated scaffolding.

Use of Synthetic Biology:
The definition of Synthetic Biology above is presented by SynbiCITE demonstrates how Synthetic Biology emphasises the redesign and ab initio design of biological systems. Our project aims to design novel mussel-foot protein parts with widespread applications - a process that necessitates a variety of Synthetic Biology techniques. Firstly, our aim is to create numerous parts that facilitate efficient production of our chosen MFP, Pvfp-5β, as well as its polymerisation and development into a polymer. To do so, we built upon a previous software that was developed by iGEM Calgary in 2019, iGAM. Although we did not use iGAM this year, we will use it next year with Wet Lab data. During the second phase of our project, we will improve the stability of our protein through consensus design as well as the adhesion of our protein using phage display libraries. Therefore, we will use a process of rational design to improve the function of our protein. Once our team has lab access we will validate the effectiveness of our model and evaluate the protein’s adhesiveness using cell adhesion assays. In this case, our team intends to use Synthetic Biology to design a novel protein with adhesive properties that can be utilised in a variety of circumstances and is a step forward in the process of creating mussel-inspired bioadhesive materials. We will be designing a system by which our protein can be produced and polymerised via a tyrosinase enzyme-based system in vitro. In doing so, we will mimic natural means of polymerisation demonstrated by mussels. Therefore, we will construct a system that can be employed for the other bioadhesive applications of our polymer beyond that of treating SCI.
References
- Badhiwala, J.H., Wilson, J.R. & Fehlings, M.G., 2019. Global burden of traumatic brain and spinal cord injury. The Lancet Neurology, 18(1), pp.24–25.
- Chai, Q., Jiao, Y. & Yu, X., 2017. Hydrogels for Biomedical Applications: Their Characteristics and the Mechanisms behind Them. Gels, 3(1), p.6.
- Katoh, H., Yokota, K. & Fehlings, M.G., 2019. Regeneration of Spinal Cord Connectivity Through Stem Cell Transplantation and Biomaterial Scaffolds. Frontiers in Cellular Neuroscience, 13.
- Migliorini, C., Tonge, B. & Taleporos, G., 2008. Spinal Cord Injury and Mental Health. Australian & New Zealand Journal of Psychiatry, 42(4), pp.309–314.
- Patek, M. & Stewart, M., 2020. Spinal cord injury. Anaesthesia & Intensive Care Medicine, 21(8), pp.411–416.
- Shrestha, B. et al., 2014. Repair of injured spinal cord using biomaterial scaffolds and stem cells. Stem Cell Research & Therapy, 5(4), p.91.
- Silva, N.A. et al., 2014. From basics to clinical: A comprehensive review on spinal cord injury. Progress in Neurobiology, 114, pp.25–57.
- Straley, K.S., Foo, C.W.P. & Heilshorn, S.C., 2010. Biomaterial Design Strategies for the Treatment of Spinal Cord Injuries. Journal of Neurotrauma, 27(1), pp.1–19.









